
Parliament
WHY CORONAVIRUS WILL BECOME AFRICA’S CATASTROPHE
By Omoshola Deji
Coronavirus disease (Covid-19) is giving humanity its toughest challenge since 1918 – when influenza killed more people than during World War I. Since its outbreak late last year in Wuhan, China, Covid-19 has infected over 3.3 million persons and killed more than 234,000 globally. The fatality keeps mounting as the virus is alive in every region, except Antarctica.
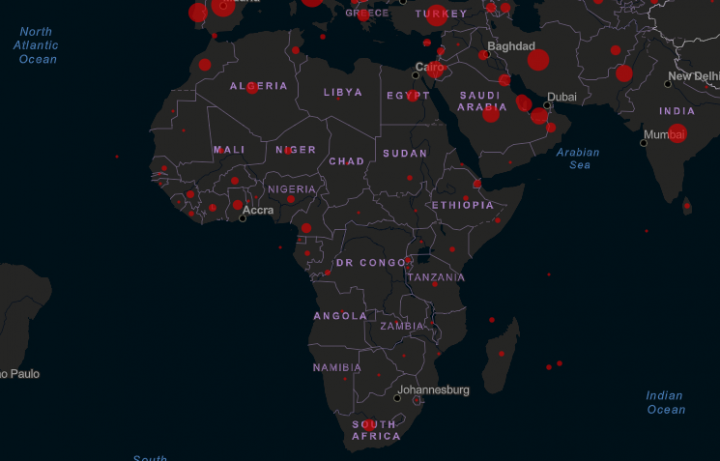
As of May 01, in order of fatality, Europe announced over 1.4 million confirmed cases and 132,543 deaths. The region of the Americas declared over 1.2 million cases and 74,591 deaths. Additionally, the Middle East announced 176,928 cases and 7,304 deaths. Western Pacific reported 146,720 cases and 6,037 deaths. Furthermore, South-East Asia reported 51,351 cases and 2,001 deaths. Africa reported 36,743 cases and 1,591 deaths, according to Statista.
Observe that Africa is the least affected continent, despite being the poorest in health care delivery and disaster control. Here we examine the factors that will make Covid-19 a catastrophe in Africa.
Late Detection
Virtually every nation on the continent lack sufficient testing facilities. The most populous nation, Nigeria has only 17 testing laboratories for about 200 million population living in 36 states and the federal capital. The labs can only conduct about 3,000 scans daily. Hence, thousands of suspected cases face a long wait. During the delay, most of the suspected cases, out of faith that they’re uninfected with Covid-19, continues to interact and infect people. Many would have stayed at the isolation centers, but the abodes are at best unconducive, and at worst inhabitable.
The late detection problem is made worse by elites using their influence to get tested fast, even when they have no reason to worry. They are robbing those who really need testing and treatment of attention. In consequence, Sudan’s first case was reported posthumously. Another posthumous case was reported in Nigeria.
False Statistics and Underreported Cases
Late detection brings about underreported cases. The low fatality being reported across Africa is deceptive. The figures gives African governments a pass mark when they’re failing. It makes them think they’re curtailing the virus excellently, when they’re not. False statistics is misleading African nations to plan poorly for an imminent outbreak. They are planning a bit ahead, when they should be planning far-ahead.
Worrying, Africa can’t measure up when the fatality erupts. The Commissioner for Health of Lagos State, Nigeria, Professor Akin Abayomi, stated during a media briefing on April 06 that “if we see 5,000 cases in four weeks or two weeks, we do not have the capacity to cope with that and most other (African) countries do not have the capacity to cope with that.”
Illiteracy and Ignorance
Majority of Africa’s rural population and the urban underclass either thinks Coronavirus does not exist or they’re immune to it. Efforts by civil societies to convince them otherwise has been abortive, and would remain so till they begin to see people die in their environment. Then, it would be too late to contain the spread.
African governments have largely failed to provide consistent and credible information to the ignorant many – a flaw the Coronavirus-5G controversy has shown some developed nations are also guilty of. Countless persons in Nigeria’s 20 million commercial city, Lagos, thinks Covid-19 is a sham. Same applies to Accra, Abidjan, Johannesburg and many others.
Majority of the rural population don’t even know what a virus is. Enlightenment is being done on the radio and television they have no electricity to power. Nationally, the illiterates and ignorant-many can’t learn online as they’re either unskilled to surf the web, lack access to internet or can’t afford it. With multitudes either discounting or ignorant of Covid-19, Africa becoming Italy is just a tick away.
Self-medication and Misdiagnosis
A lot of people guess ailment, and treat themselves when sick in Africa. This act is mainly caused by illiteracy, poverty, unaffordable, and unavailable health care services. People who periodically suffer from ailments that share symptoms with Covid-19 will naturally think they’re down with the same ailments when sick. Several persons on the continent are currently treating cough, malaria, and other common illnesses when they are actually down with Covid-19.
Africans rarely visit hospitals to treat common ailments such as cough and malaria. They simply procure a widely-acclaimed effective drug or make herbal concoctions for cure. It is when the self-medications fail that they think of hospital. In the course of misdiagnosis and self-medication, they infect their contacts, who then go on to infect the larger community. Such delay in diagnosis and treatment is what Covid-19 needs to spread.
Rife Malnutrition and Terminal Diseases
Africa has infectious pathogens such as Lassa hemorrhagic fever and Ebola. The continent also has several people living with deadly diseases such as cancer, tuberculosis and HIV. There are roughly 15.3 million people living with HIV in Africa, according to the World Health Organization (WHO). Covid-19 will exterminate these immune compromised persons fast, if they contract it. South Africa has over 7 million HIV-infected persons.
Tuberculosis weaken the lungs, which make its patient who contract Covid-19 susceptible to death. WHO reported 2.5 million persons fell ill with tuberculosis in Africa in 2016. This implies that the continent currently has no less than 10 million persons living with tuberculosis.
Than other continents, Africa has scores of youngsters whose supposed strong immune should hasten recovery from Covid-19. Unfortunately, many are suffering from malnutrition due to pervasive poverty. The malnutrition, which has weakened their immune system, would make them die fast of Covid-19.
Deficient Infrastructure
One means of preventing Covid-19 spread is regular hand washing, but potable water supply is a challenge in most parts of Africa. There are three prevailing conditions in the cities: water is either being rationed, sourced from private boreholes, or purchased daily. Buying water to wash hands regularly is unrealistic to the poor majority living in slums. They also can’t afford sanitizers due to price hike.
Electricity is a problem. Employees told to work from home are unable to function due to lack of power. Rather than work, people spend most part of the day discussing. Those already infected, but asymptomatic, spread Covid-19 while passionately talking sports, politics, fashion, etc. Some go out to play football. Such action, influenced by infrastructural deficiency, aids community transmission.
Beyond the metropolis, the rural areas are worse off as some parts have no infrastructural exposure. The lack of amenities will frustrate the fight against Covid-19 as poor living conditions will make people have close interaction, even if they don’t wish to.
Uncontrollable Spread in Vulnerable Communities
Extremely poor persons in Africa think abroad returnees are wealthy. As a result, many would have beseeched the infected returnees for alms and contracted Covid-19. Regrettably, these poor persons have returned to their densely populated communities spreading the virus.
Furthermore, some of the returnees who tested positive have hangout at popular spots and visited their relatives in the village. One thing African villages – most of which lack health facilities – need to go in ruins is a single case of Coronavirus. Several cases have been recorded in many villages.
Also vulnerable are the internally displaced persons and refugee camps. According to estimates by the United Nations Refugee Agency (UNHCR), eight of the world’s ten largest refugee camps are located in Africa and occupied by 6.3 million persons. Almost 18 million persons are internally displaced across the continent. People living in close proximity, as experienced in the displaced and refugee camps, have a high risk of contracting Coronavirus. Just one sneak-in case will cause disaster. Same for the overly congested prisons.
Impracticable Social Distancing and Self-Isolation
Curbing Covid-19 via social distancing and self-isolation is only effective in other continents, where majority of the population have descent homes. In Africa, except the rich few, people generally live close together, sharing toilet and bath. Over 40 people share convenience in some densely populated homes. Under such condition, how would a couple occupying a room with four children practice social distancing? Should one of them get infected, how would (s)he self-isolate?
African cities are congested out of rural-urban migration and the search for job opportunities. The rural migrants, many of whom can’t afford to own a home in the city, live in uncompleted buildings. Some team up to rent an apartment. A few of the migrants save to own an apartment and sublet bed spaces. The sleeping pattern in those apartments is synonymous to the prisons. How would such plebs in Abidjan, Cape Town, Nairobi, Lagos and other cities practice social distancing? All Coronavirus needs to rule there is just one victim, and now it has many.
Hasty Ease of Lockdown
Africa has taken raft measures to curb Covid-19, but if the fatality witnessed in leading continents is anything to go by, the black race cannot escape a catastrophe. Despite being disadvantaged, African nations are easing lockdown to save their economies, while the most part of other continents remain lockdown. This will lead to an aggravation of fatality. In fairness to Africa, America and Europe have strong economies to float prolonged lockdown, but Africa do not. Thus, the continent is trapped between a rock and a hard place – remain on lockdown to save lives or ease out to save the economy.
Opting for the economy will bring Africa catastrophe. The most populous nation, Nigeria is relaxing lockdown amid fast rising Covid-19 cases. Nigeria failed to learn from Ghana, whose infection rose tremendously a week after relaxing lockdown. Africa’s hasty ease of lockdown, especially in the congested cities – where social distancing and hygiene devotion is almost impossible – is the havoc wreaking opportunity Covid has been seeking. The easement won’t last as increased fatality would lead to restoration of lockdown.
Poor Healthcare System
African countries healthcare system lacks capacity. WHO recommends doctor-population ratio of 1:1,000, but Cameroon, Central African Republic, and Somalia has 1:10,000. Kenya has 130 intensive care unit (ICU) beds for 50 million people. South Africa has 3,500 ICU beds for 58 million population – a three quarter of what Italy with similar population has.
Nigeria has 350 ICU beds for 200 million people. Most of the nation’s healthcare facilities don’t have clean running water. Generally, the system is so flawed that doctors had to call off strike over unpaid wages to combat Coronavirus.
Other challenges rendering African healthcare systems incapable of handling several Covid-19 cases include low budgetary allocation, poorly paid staffs, and equipment shortages. The hospitals lack sufficient test kits, laboratories, ventilators, masks, gloves, medicines, protective suits, and other essentials. These deficiencies put Africa in a tragedy of not being able to fend for itself as the Covid-19 cases multiply.
End Note
Except an existing drug, such as the Chloroquine being touted by US President Donald Trump works, or the newly discovered vaccines on trial come out effective, Africa cannot escape a catastrophe. A direful state in which many will die without doctor’s touch is looming. Thousands will rest eternally in mass graves. It’s difficult for optimists to accept and painful for the writer to assert, but the handwriting on the wall is as clear as the biblical “Mene, Mene, Tekel, Upharsin.” Covid-19 will deliver its message of catastrophe to Africa in the next days.
*Omoshola Deji is a political and public affairs analyst. He wrote in via moshdeji@yahoo.com


Oche Nehi
There was a time in Nigeria when securing a job marked the beginning of a better life. Employment meant stability, dignity, and hope. Parents sacrificed everything to educate their children because they believed a certificate would open the door to prosperity. That social contract has now been broken.
Today, millions of Nigerians rise before dawn, endure hours of traffic, work eight to twelve hours daily, and still return home unable to provide decent meals, pay school fees, settle rent, or save for tomorrow. They are not unemployed. They are not lazy. They are victims of an economy that increasingly punishes honest labour while rewarding political privilege.
Nigeria has quietly created a new class of citizens the WORKING POOR.
This silent emergency deserves as much national attention as unemployment, insecurity, and corruption because it is gradually eroding the dignity of work itself.
Across ministries, hospitals, schools, banks, factories, media houses, security agencies, and private businesses, countless workers now live from one salary to the next. For many, the salary is exhausted within days of payment. The remaining weeks are financed through borrowing, cooperative societies, digital loan apps, family support, or pure endurance.
The consequences are visible everywhere.
- A teacher who educates the nation’s future cannot afford quality education for her own children.
- A nurse entrusted with saving lives struggles to pay hospital bills when illness strikes her family.
- A police officer charged with protecting society battles to feed his household.
- A journalist exposing corruption cannot afford decent housing.
- A junior civil servant, after paying rent, transportation, electricity bills, food, and other essentials, is left with little or nothing before the next payday.
These are not isolated stories. They represent a growing national reality.
The tragedy is that Nigerians are working harder than ever before, but getting poorer with every passing year.
The reasons are not difficult to identify. Inflation has steadily reduced the value of wages. Food prices have reached levels unimaginable just a few years ago. Transportation costs have surged. House rents continue to climb in major cities. Electricity tariffs and other basic living expenses consume increasing portions of household income. Yet salaries particularly in the public sector and among lower-income workers in the private sector have failed to keep pace with these rising costs. The result is predictable: employment no longer guarantees economic security.
This should alarm every policymaker.
When workers can no longer afford the basic necessities of life despite full-time employment, productivity declines, corruption becomes more tempting, brain drain accelerates, and public confidence in government weakens.
Perhaps the greatest danger psychological. A generation that believes hard work no longer leads to progress is a generation that begins to lose faith in legitimate enterprise. It is no coincidence that more young Nigerians now dream of leaving the country than building careers within it. They are not simply chasing higher salaries abroad; they are searching for societies where effort is rewarded and work restores dignity.
At SecretsReporters, we believe this crisis cannot be separated from governance. While governments at various levels have introduced reforms intended to stabilize the economy and improve public finances, ordinary Nigerians continue to judge success by what happens in their kitchens, not by what appears in policy documents. Economic reforms that fail to translate into improved living conditions will inevitably face questions from the citizens they are meant to benefit.
This is why accountability must extend beyond budget speeches and official statistics. It must answer a more fundamental question:
Why are Nigerians working harder but living poorer? The answer demands honesty. It requires confronting inflation, improving productivity, investing in affordable public transportation, expanding access to quality healthcare and housing, supporting businesses that create decent jobs, and ensuring that wage policies reflect the real cost of living.
It also requires government at every level to recognise that development cannot be measured solely by infrastructure projects or macroeconomic indicators. A nation succeeds when ordinary workers can afford food, educate their children, access healthcare without financial ruin, and retire with dignity.
Employment should be the strongest weapon against poverty not another expression of it.
The working poor are not asking for luxury. They are asking for fairness. They seek an economy where honest work can provide a decent life and where sacrifice is rewarded with opportunity rather than perpetual hardship. Nigeria cannot continue to celebrate employment figures while ignoring the quality of life of those who are employed. A job that cannot feed a family, pay rent, or meet basic human needs is no longer a pathway out of poverty it is evidence of a deeper structural failure.
As this newspaper has consistently maintained, the true wealth of any nation is not measured by the fortunes of a privileged few but by the dignity enjoyed by its ordinary citizens. The millions of Nigerians who keep this country running teachers, nurses, artisans, factory workers, journalists, drivers, civil servants, farmers, traders, and security personnel deserve more than applause for their resilience. They deserve an economy that values their labour. The greatest injustice in today’s Nigeria is not merely that many people cannot find jobs.
It is that millions who already have jobs are still living in poverty.
That should trouble every leader. And it should trouble every Nigerian.

By Barau Simon (Dantani Jr)
When he took office as the Minister of Health and Social Welfare Prof. Muhammad Ali Pate made a bold promise: to “Save Lives, Produce Health, and do it for all Nigerians.
But as bold as his promises are and were, the decline of the Nigerian health sector, as well as the dwindling of it, has shown that the Minister’s assertion while taking office was just mere words and rhetoric and has not at any point translated into realities and achievements of any sort.
A cursory look at the just-verbalized four-pillar agenda he dished out to revamp the health system shows that, rather than delivering, the health system has been in a comatose state.
What he promised and what the reality is at the moment:
He promised the health governance and synergy, pledging to coordinate the three tiers of government, the health sector has continued to battle a historical lack of synergy between federal, state, and local governments, fragmentation has been the word that is existing in this sector, as it is this has brutally hampered primary healthcare (PHC) delivery, resulting in overloaded tertiary hospitals, poor funding, and inadequate supply of medical staff and supplies across rural communities.
On the ground, realities prove that the “lack of synergy” remains an ongoing hurdle, which is a slap on the minister’s promise of health governance synergy. Under him, stakeholders have often pointed out that needs assessments of the community are hardly or not even synchronised, an act that has led to duplications in some areas and complete neglect of medical facilities in others.
Again, he promised Primary Healthcare (PHC) and Maternal Health, the minister’s assertion to focus on expanding and revitalizing grassroots primary care to ensure basic services—such as routine vaccines and maternal health facilities—are available to everyone has remained a mirage; nothing has been achieved further than what was achieved in the previous governments.
As of today, the primary healthcare (PHC) system in Nigeria is relentlessly constrained, with only about 20% of the over 30,000 PHC facilities deemed fully functional. There is little or no funding, and the continuous massive brain drain of medical professionals, dilapidated infrastructure, and severe shortages of essential drugs and medical equipment remain unchanged.
The case of six in ten Nigerians lacking access to quality primary health care service remains as it is, there has not been any improvement under the current minister and with the basic primary facilities lacking delivery tools, emergency interventions, and skilled midwives, treatable pregnancy complications regularly turn fatal, particularly for women and newborns in rural communities, and so far so long, maternal and child mortality has remained even high more than the way it is before he took saddle on the position as the minister.
Suffice to say that the Nigerian health sector, under the Coordinating Minister of Health and Social Welfare Prof. Muhammad Ali Pate, instead of soaring high like what he promised when he took office, is rather plummeting, and this is shown in terms of severe infrastructural decay, paralyzing labor strikes, and systemic vulnerabilities that have continued.
Key areas that show failure in the health sector under Ali Pate
Decay of Facilities
Little or no funding has left tertiary health institutions brutally derelict, as seen in the dilapidation of diagnostic and laboratory facilities within them, which has shifted the weight of apt medical investigations to costly private hands.
Labour Strike and Crisis of Human Resources
There have been a series of strikes embarked by health workers and medical personnel under Ali Pate as Minister of Health. More so, there have been obnoxious policies that have exacerbated the human resource crisis and sped the “brain drain” of medical professionals leaving the country in droves.
They are as follows;
Non-payment of Entitlements: The health sector has been plagued by incessant and interminable strikes by medical workers, including the Nigerian Association of Resident Doctors (NARD), the Joint Health Sector Unions (JOHESU), demanding the implementation of the Consolidated Health Salary Structure (CONHESS).
The Minister’s “No Work, No Pay” Policy: Under the Minister’s leadership, his ministry enforced an abhorrent rule of a “no work, no pay” for striking health professionals, a posture health sector critics argued has worsened the human resource crisis and sped the “brain drain” of medical professionals leaving the country in their numbers.
Professor Muhammad Ali Pate’s enforcement of the “no work, no pay” rule for striking health workers—particularly during the prolonged 2025–2026 Joint Health Sector Unions (JOHESU) industrial action over the Consolidated Health Salary Structure (CONHESS)—severely disrupted public healthcare delivery.
Service Disruption: The policy failed to deter unions like JOHESU, which represents roughly 85% of the healthcare workforce. Workers continued their strike, forcing public hospitals to close or operate at heavily reduced capacities, leading to delayed treatments, postponed surgeries, and compromised patient care.
Worsening Brain Drain: Financial pressures, combined with a lack of hazard allowances and delayed wage negotiations, are accelerating the exodus of vital health workers. This “japa” wave leaves the remaining public hospitals critically understaffed.
Deteriorating Sector Morale: The enforcement of this rule—which was applied to some unions but selectively missed for others—has bred feelings of marginalization and institutional disrespect. Experts warn that these execution gaps and disputes undermine trust in the government’s ability to manage health system reforms.
Increased Out-Of-Pocket Costs: With public hospitals paralyzed by these labor disputes, vulnerable Nigerians have been forced to bear the high, out-of-pocket costs of seeking care at private clinics.
The hidden cost of these prolonged labor disputes ultimately cripples the population’s access to care, with citizens bearing the brunt of the instability.
How Health Policies Are Fragmentally Executed As Gaps Exist In Policy Implementation
Feeble and Weak Execution: for instance, health sector Groups like Corporate Accountability and Public Participation Africa (CAPPA) have mentioned failures to execute health funding policies as a reason for frequent expenses and overdue care for patients.
Struggles within the State Level: Despite policies being made, the Nigerian Health sector critics are of the view that even with reforms and policies, little or nothing has been implemented successfully in the states.
Continuous Brain Drain Syndrome Under The Minister
In February 2025, the Minister of Health for the State, Professor Iziaq Salako, reechoed what his boss, Professor Ali Pate, has consistently said of stopping the brain drain syndrome, popularly known as japa syndrome.
But the reforms under the Minister of Health Professor Ali Pate have failed to arrest or stop the japa syndrome, even with targets to increase local medical manpower and retain professionals. Persistent inflation, poor remuneration, and challenging working conditions have continued to drive record numbers of Nigerian health workers to migrate.
Critics and unions argue these measures do not address the root causes of the japa wave, they said poor foundational salaries and systemic lack of infrastructure continue as the primary drivers of the brain drain.
Non-payment of entitlements, policy somersault has continued to cause industrial actions by health and medical personnel.
Timeline of strikes under the current Minister of Health
Under the tenure of the Coordinating Minister of Health and Social Welfare, Prof. Muhammad Ali Pate, the Nigerian Association of Resident Doctors (NARD) engaged in a prolonged strike in late 2025 and issued several ultimatums in 2026 over unfulfilled welfare and allowance agreements.
The timeline of major NARD industrial actions and agreements under his administration includes:
•July 2023: NARD embarked on a nationwide, indefinite strike over unfulfilled salary and allowance demands. The action lasted until mid-August.
In November 2023, President Bola Tinubu approved the waiver of the “No Work, No Pay” order against the doctors.
•September 2025: NARD issued a 30-day ultimatum to the Federal Government regarding lingering welfare issues, specifically the non-disbursement of the 2023 Medical Residency Training Fund and unpaid arrears.
•November 1, 2025: Following the expiration of ultimatums, NARD began a “total, comprehensive and indefinite” nationwide strike over overwhelming workloads, unpaid salary arrears, and poor hospital infrastructure.
•November 29–30, 2025: NARD signed a 19-item Memorandum of Understanding (MoU) with the Federal Government. The union’s National Executive Council voted to suspend the 29-day strike to allow government ministries to fulfill commitments.
•January 12, 2026: NARD resumed its indefinite strike, citing the Ministry of Health’s failure to implement provisions from the November MoU (such as correcting professional allowance errors and reinstating dismissed union leaders in Lokoja) and the enforcement of a “no work, no pay” policy.
•February 2026: The broader health sector experienced significant friction, as JOHESU embarked on a strike.
•April 7, 2026: NARD initiated another nationwide indefinite strike due to protracted pay disputes and the government’s attempts to halt the newly revised Professional Allowance Table (PAT).
•April 8, 2026: Following high-level interventions by Vice President Kashim Shettima and Minister Pate, NARD suspended its indefinite strike after the government committed to restoring the revised allowance table.
Under Professor Ali Pate as Health Minister, the Joint Health Sector Unions (JOHESU) embarked on two major industrial disputes and other ones all these are primarily driven by demands for the implementation of the adjusted Consolidated Health Salary Structure (CONHESS) and other welfare packages.
A timeline of these actions:
•June 2023: Health workers embarked on a 12-day nationwide strike. The action was suspended after a direct intervention by President Tinubu, who requested a 21-day timeline to resolve the unions’ demands. [1]
•November 2025 – February 2026: Following prolonged stalemates regarding the full implementation of the adjusted CONHESS, JOHESU declared an indefinite nationwide strike on November 15, 2025. The strike paralyzed public tertiary and secondary health institutions nationwide.
•January 2026: The Federal Government invoked the “No Work, No Pay” policy in an attempt to force striking health workers back to their duties, a move the union strongly resisted.
•February 2026: Following successful conciliation meetings in Abuja with the Federal Ministry of Health and Social Welfare, JOHESU officially suspended their 84-day nationwide strike on February 6, 2026.
Also under him, the National Association of Nigerian Nurses and Midwives (NANNM) has embarked different strikes action over disputes that centers on salary structure adjustments, inadequate staffing, and unpaid allowances.
A detailed timeline of these actions is as follows:
July–August 2025: Nationwide Warning Strike
•July 14, 2025: Nurses issued a 15-day ultimatum to the federal government citing poor remuneration, staff shortages, and unresolved welfare issues. [1, 2]
•July 30, 2025: Following the expiration of the ultimatum, nurses commenced a 7-day nationwide warning strike that temporarily paralyzed health services at 74 federal hospitals, state facilities, and primary health centers. [1, 2]
•August 3, 2025: NANNM suspended the warning strike after the federal government signed a Memorandum of Understanding (MoU) with agreed-upon timelines for addressing key demands, including the gazetting of a new scheme of service and finalizing the upward review of allowances.
Mid-2026: Continued Unrest and Negotiations
•May–June 2026: Lingering distress over delayed allowances, coupled with Nursing and Midwifery Council of Nigeria (NMCN) certificate delays, continued to generate unrest in the sector. Negotiations over the new allowance structures and demands to implement full agreements remain ongoing, with unions frequently warning of further industrial action to press home their demands.
Grants Received
As the Coordinating Minister of Health and Social Welfare, Prof. Muhammad Ali Pate, Nigeria has received and facilitated over $4.6 billion in foreign health grants and investments. Key international funding received under his tenure includes:
• Global Fund: An allocated $933 million grant for the implementation period spanning across 2024 to 2026 to combat HIV/AIDS, tuberculosis, and malaria.
• United States Government: A nearly $2 billion grant commitment to support Nigeria’s health priorities, specifically focusing on antiretroviral therapies, malaria, and maternal/child health.
• International Investment & Localization: Over $5.5 billion in foreign investments have been secured to build local pharmaceutical and healthcare manufacturing capacity, including financing from the European Investment Bank and Afreximbank.
Despite grants received, cases such as Malaria, Tuberculosis has remained high. Nigeria remains vulnerable to recurring disease outbreaks, exposing the weakness of its healthcare system.
Nigeria’s health sector remains fragile despite the Minister’s so much talk of bold promises and what he has achieved under the sector that are nowhere to be seen.
Even with his policy and reforms the persistence of challenges still rearing their ugly heads health sector raises questions about his capacity to improve healthcare in Nigeria as he has claimed he will do.
For instance at the 2025 Strategic Health Summit, health advocates assessed the sector’s progress and acknowledged that significant gaps persist.
Ali Pate’s approach to healthcare sector where he superintend as the Minister has become a mix of broken promises and penny-pinching. The consequence is simple and brutal. For Nigerians, visiting a public hospital has become a gamble. Will you see a doctor? Will the lab be open? Will the nurse be available? Will the strike still be on?
And even if you are lucky, you are likely to meet exhausted professionals carrying the weight of a system that refuses to support them.
This is the state of our public healthcare under the current Minister.

Dr David Ejiofor
To understand why Nigeria’s Minister of health Prof Muhammad Ali Pate has an umbilical like linkage to Bill Gates one will have to unravel the motive behind the multimillion dollar support from Gates foundation, the reason may not be far fetched over the years experts have theorized that Gates has been behind harmful medical experimentation around population control in Africa and Nigeria especially. And Pate is his gateway to ensure a massive population control. To stop Nigeria from becoming the third most populous country by 2050. This may sound far fetched to the undiscerning but there’s a precedence to this.
Public skepticism toward foreign-funded medical initiatives in Nigeria cannot be understood without reference to the 1996 Pfizer Trovan trial in Kano. During a meningitis outbreak that claimed thousands of lives, Pfizer tested the experimental antibiotic Trovan on children. Subsequent investigations and legal disputes raised serious concerns regarding informed consent procedures, ethical approvals, and research oversight. The controversy left a lasting impact on public trust and remains one of the most cited examples of ethical failures in medical research conducted in developing countries.
The legacy of the Trovan case continues to shape public perceptions of international health interventions. For many Nigerians, it serves as a reminder of the need for rigorous safeguards whenever foreign-funded research or medical programs involve Nigerian citizens.
Western-sponsored vaccines have thus become tools for population control with Gates Foundation at the forefront. More recently, discussions on social media and other online platforms have revived concerns about transparency, accountability, and oversight in international health collaborations. While various claims and allegations have circulated online, many remain unverified and should be treated with caution unless supported by credible evidence and official investigations.
Nevertheless, the broader questions raised by citizens deserve serious consideration. Nigerians have a legitimate interest in knowing that all medical research, health interventions, and international partnerships affecting their wellbeing are conducted in accordance with the highest ethical standards.
In this regard, health policy experts emphasize the importance of strong regulatory institutions, informed consent procedures, independent ethical review boards, and transparent government oversight. Public confidence in healthcare initiatives depends not only on scientific effectiveness but also on trust, accountability, and respect for human dignity.
A few months ago verified emails, circulated online analyzing and measuring women’s bodies and possible medical imaging. Among these were email exchanges said to be between Epstein and the same Gates, where specifically mentioned Nigeria and their anatomy, in which he was reportedly requested to bring women from Nigeria, with suspicions raised that parts of their bodies might be used for activities linked to potential research that may be contravenes the Nuremberg code of medical research ethics.
For many observers, the debate is ultimately about safeguarding the rights of citizens under principles that have guided medical ethics since the Nuremberg Code. No foreign-funded research involving Nigerians should proceed without fully informed consent, rigorous ethical scrutiny, and transparent government oversight. Anything less risks undermining public trust and repeating mistakes that history has already warned against.
As Nigeria deepens its engagement with global health partners, the challenge is not to reject international cooperation but to ensure that such partnerships operate under robust safeguards that protect the rights and interests of Nigerian citizens. Transparency, public accountability, and ethical compliance must remain at the heart of every health intervention conducted within the country.
Ultimately, the debate reflects a broader global issue: how nations can benefit from international scientific collaboration while maintaining sovereignty, public trust, and rigorous protection of their citizens.
-
 STRAY BULLET10 years ago
STRAY BULLET10 years agoYOU ARE A THIEF SO YOU CAN’T PROBE A THIEF: ANOTHER UK NEWSPAPER WRITES BUHARI
-
 LATEST NEWS10 years ago
LATEST NEWS10 years agoPREACH AND DIE: FOR DARING EARLY MORNING PREACHING IN ABUJA, MUSLIMS HACK TWO PASTORS TO DEATH
-
 LATEST NEWS9 years ago
LATEST NEWS9 years agoBREAKING: TYRANNICAL NIGERIA PRESIDENT, MUHAMMADU BUHARI DIES IN LONDON HOSPITAL, BUT PRESIDENCY KEEPS SEALED LIPS
-
 SPECIAL REPORT10 years ago
SPECIAL REPORT10 years agoMISS ANAMBRA CUCUMBER SAGA: HOW ANAMBRA BROADCASTING SERVICE DIRECTOR, UCHE NWORAH LEAKED SEX VIDEO TO THE PUBLIC FOR HER REFUSAL TO CONTINUE SEXUAL AFFAIR WITH HIM (PART ONE)
-
 SPECIAL REPORT10 years ago
SPECIAL REPORT10 years agoEXCLUSIVE: HOW STEPHEN KESHI AND WIFE WERE KILLED BY HIS OWN BROTHER
-
 SPECIAL REPORT9 years ago
SPECIAL REPORT9 years agoPOWER GAME ALMOST OVER: OSINBAJO UNDER PRESSURE TO HAND OVER TO SARAKI AS VP IN ANTICIPATION OF THE UNKNOWN
-
 STRAY BULLET10 years ago
STRAY BULLET10 years agoDESPITE HUNGER IN NIGERIA, BUHARI ALLEGEDLY DONATES 500 MILLION DOLLARS TO HILARY CLINTON’S FAILED PRESIDENTIAL ELECTIONS AS NIGERIANS PRESSURE HIM TO CONGRATULATE TRUMP
-
 SPECIAL REPORT10 years ago
SPECIAL REPORT10 years agoEAR INFECTION SCAM: BUHARI JETS TO LONDON TO SECRETLY NEGOTIATE WITH NIGER DELTA AVENGERS